Introduction
- Overview
-This approach can be a fairly extensile exposure, allowing
access to the anterior, medial, and lateral aspects of the shoulder.
-This approach is done in a supine position with a roll or
wedge under the medial scapula.
- Indications
- Proximal humerus fractures
- Long head of the biceps injury
- Reconstruction of recurrent dislocations
- Septic glenohumeral joint
- Shoulder arthroplasty

Internervous plane
- Deltoid
muscle (axillary nerve.)
- Pectoralis
major (medial and lateral pectoral nerve)

Approach
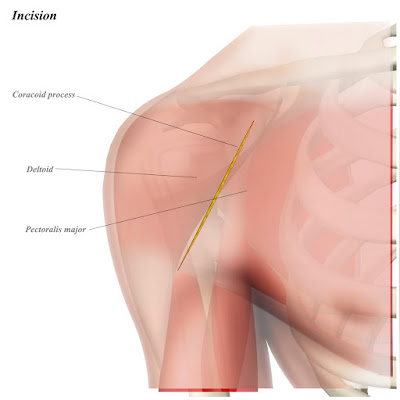
- Incision
- An incision is made following the line of the
deltopectoral groove
- In obese patients, this may be difficult to
palpate; the incision starts at the coracoid process, which is usually more
easily palpable
- A 10-15 cm incision is usually utilized, but is
sized according to surgical need and size of patient

- Superficial dissection
- Attention must be paid to superficial skin
vessels, as these can bleed significantly
- The
deltopectoral fascia is encountered first ;
the cephalic vein is
surrounded in a layer of fat and is used to identify the interval
- The cephalic vein can be mobilized either
medially or laterally, depending on patient factors and surgeon preference.
- Fibers of the deltoid are retracted laterally
and the pectoralis major is retracted medially


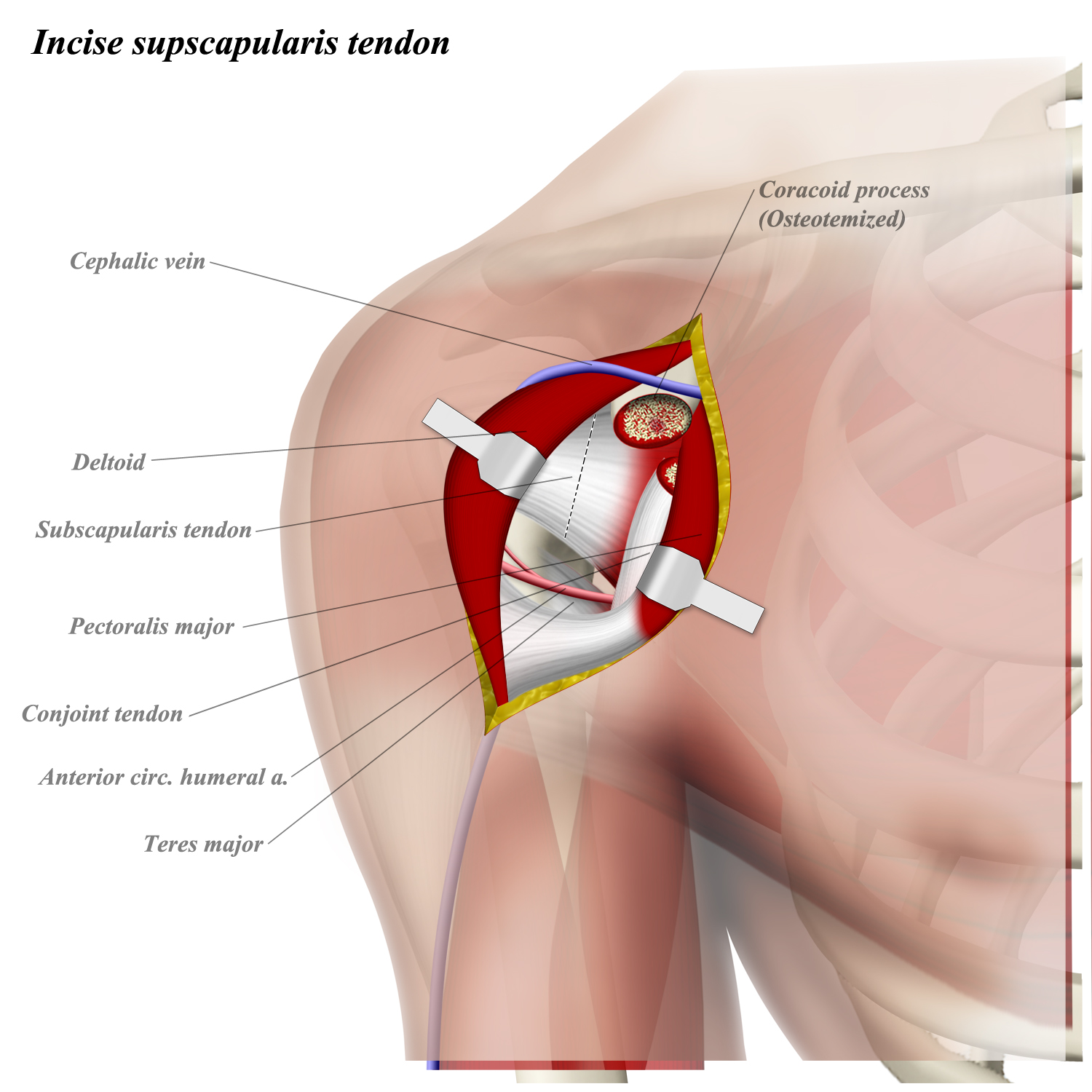
-Deep dissection
- The short head of the biceps and
coracobrachialis arise from the coracoid process and are retracted medially.
- The musculocutaneous nerve enters the biceps
5-8cm distal to the coracoid process; retraction of the conjoint tendon must be
done with care.
- The fascia on the lateral side of the conjoint
tendon is incised to reveal the subscapularis
-External rotation puts the subscapularis fibers
on stretch
- The subscapularis may be released from its
insertion on the lesser tuberosity through the tendon or via an osteotomy
- The capsule is then incised (as needed) to
enter the joint


Dangers
- Musculocutaneous
nerve
-Renters medial side
of biceps muscle 5-8 cm distal to coracoid (stay lateral)
-Can have neuropraxia
if retraction is too vigorous
- Cephalic
vein
-Should be preserved
if possible; if injured, can ligate
- Axillary nerve
-At risk with release of subscapularis tendon
(runs distal to) or with incision of teres major tendon or latissimus dorsi
tendon (runs proximal to)
- Anterior
circumflex humeral artery
Runs
anteriorly around the proximal humerus cephalad to pectoralis major tendon

0 comments:
Post a Comment